Cooperativismo y Desarrollo, May-August 2020; 8(2), 315-328
Translated from the original in Spanish
Enterprise social responsibility and competitiveness in private health clinics in Quito, Ecuador
Responsabilidad social empresarial y competitividad en las clínicas de salud privadas de Quito, Ecuador
Responsabilidade social das empresas e competitividade nas clínicas de saúde privadas em Quito, Equador
Bryan Roberto Grijalva Morejón1, Angie Fernández Lorenzo2
1 Universidad de las Fuerzas Armadas - ESPE. Ecuador. ORCID:
https://orcid.org/0000-0003-4845-2885. Email: brgrijalva@espe.edu.ec
2 Universidad de las Fuerzas Armadas - ESPE. Ecuador. ORCID:
https://orcid.org/0000-0001-6106-8576. Email: angie821218@gmail.com
Received: July 9th, 2020.
Accepted: August 11th, 2020.
ABSTRACT
Enterprise Social Responsibility aims to link the enterprise with its internal and external actors with adequate professional practices, outlining the role of the organization, both in economic and social activities. A descriptive correlation research was carried out, applying a 9-dimensional survey, in a sample of 58 private health clinics in Quito, calculating the indexes of compliance with social responsibility and competitiveness and applying factorial analysis, in order to determine the components that denote the most important relationships between both variables. The three fundamental components defined were levels of social responsibility with active participation in the community, internal and external results of organizational structure and labor practices and innovation.
Keywords: enterprise social responsibility; competitiveness; health clinics; constructs
RESUMEN
La Responsabilidad Social Empresarial tiene como objetivo vincular a la empresa con sus actores internos y externos con adecuadas prácticas profesionales, delineando el rol de la organización, tanto en actividades económicas como sociales. Se realizó una investigación descriptiva correlacional, aplicando una encuesta de 9 dimensiones, en una muestra de 58 clínicas de salud privadas de Quito, calculándose los índices de cumplimiento de responsabilidad social y competitividad y aplicando el análisis factorial, con el fin de determinar los componentes que denotan las relaciones más importantes entre ambas variables. Los tres componentes fundamentales definidos fueron los niveles de responsabilidad social con la participación activa en la comunidad, resultados internos y externos de estructura organizacional y prácticas laborales e innovación.
Palabras clave: responsabilidad social empresarial; competitividad; clínicas de salud; constructos
RESUMO
A Responsabilidade Social Empresarial visa ligar a empresa aos seus gestores internos e externos com práticas profissionais adequadas, delineando o papel da organização, tanto em atividades económicas como sociais. Foi realizada uma pesquisa de correlação descritiva, aplicando um inquérito a 9 dimensões, numa amostra de 58 clínicas de saúde privadas, em Quito, calculando os índices de cumprimento da responsabilidade social e competitividade e aplicando uma análise fatorial, a fim de determinar os componentes que denotam as relações mais importantes entre ambas as variáveis. Os três componentes fundamentais definidos foram níveis de responsabilidade social com participação ativa na comunidade, resultados internos e externos da estrutura organizacional e práticas laborais, e inovação.
Palavras-chave: responsabilidade social das empresas; competitividade; clínicas de saúde; construções
INTRODUCTION
Enterprise Social Responsibility (RSE in Spanish) provides the enterprise with a structure of highly specialized knowledge in specific areas and activities of great importance in the organization; this opens up the possibility of employing new development strategies, an adequate use of tools, standards and norms that are on a par with the functioning of organizations (Fernández et al., 2017). RSE has become a strategic ally in: the operation of organizations, responsibility with collaborators, the community and the State, consolidating lasting relationships and urging each of its actors to become involved in the actions that these organizations carry out, among other aspects recognized by the scientific literature.
RSE is an important exercise in achieving evolution in companies, seeking to renew and mature them in the market sector in which they operate. This practice generates, in turn, reports that help to determine standards, guidelines and methodologies for the internal and external management of companies (Duque Orozco et al., 2013). The development and importance of human capital within the organization has generated new proposals on RSE that seek to encourage employees to constantly improve in the workplace, family and community, contributing to local and global improvement. RSE is an innovative form of management in organizations since it relates the company's ethics with the entities to which it is related, establishing goals that are compatible with the sustainable development of society; seeking to preserve environmental and cultural resources; thinking about and considering future generations; respecting their diversity and promoting the reduction of social inequality (Reficco & Marquina Feldman, 2015.
In the corporate environment, RSE has developed a new business philosophy, adjusting the purposes of organizations where senior management must focus on maintaining and consolidating the company's reputation, sustaining health issues for employees, consumers or clients and the community in general; this, in turn, with the objective of defining and marking a clear business competitiveness (Duarte, 2015). The organizations that are based on the principles of RSE develop a high level of business competitiveness, setting the guidelines and philosophy among their human capital, seeking to transmit stability, security, commitment and empowerment in each of their activities, thus contributing to society with responsible collaborators and exemplary citizens in terms of ethics and values.
Over the years, companies must feedback their competitiveness to face new and challenging challenges, considering factors of innovation, technology, productive flexibility and quality. The competitiveness in the organizations and their interaction in the market depends on the decisions that the people in charge of the organizations make, based on the experience, precise and quality information (Luciani Toro & Navarro Silva, 2018).
Several companies in Ecuador seek, with effort, to comply with regulations and laws on environmental treatment and investment, which is indispensable for their good operation, becoming an essential factor for companies to emphasize the dimensions that can be achieved; investment in advice to carry out and disseminate RSE reflects better financial results (Coba Molina et al., 2017). The costs involved in implementing RSE practices are a constraint on investing in programs or policy implementation. This leads to RSE becoming a management model that enables good decisions to be taken without affecting its collaborators, environment and community (Naranjo Arango et al., 2018).
Medical practices in health, by themselves, must be correct and ethical, always with the obligation to be socially responsible with their internal and external actors; health must be considered a task of governments and is shared by each sector of society, determining that this is an ethical responsibility of those involved in the sector (Ruiz de Chávez, 2016). The socially responsible approach of a public or private health institution is characterized by its capacity to identify health problems, identify strategies to solve them, and manifest the real impact that this entails.
An organization, which provides health services and which argues that it is socially responsible, must be able to present transparent results to its evaluation of operations where it is evident that no interest group is negatively affected (Gómez Perdomo, 2018).
The most convenient thing in RSE, in the field of health, is: to design and execute new approaches, new criteria and new actions that guarantee its application in health practice, science and technology, mainly seeking to eradicate the barriers of free access to the health system (Morales-Guzmán-Barró, 2014). The relationship between health and the environment from RSE approach is an incipient, very sensitive issue and one of great debate in the context of health in Ecuador, since dealing with this issue entails assuming actions, positive attitudes and, above all, responsibility towards the environment and community health (Vásquez Fajardo et al., 2018).
In the Quito Metropolitan District, new approaches to RSE have been adopted in the areas of health, with emphasis and support in the application of better and cleaner technologies in the sector, with the aim of reducing or eliminating environmental alterations, both internally and externally, and seeking to generate benefits for the actors and human groups involved, within the framework of their development and growth plans, considering both cultural and ethical aspects as well as environmental ones (Terán Rosero et al., 2017).
The objective of this research is to establish the relationship between the RES and competitiveness in private health clinics in the Quito Metropolitan District.
MATERIALS AND METHODS
The present research is of a descriptive-correlational type. Theoretical and empirical methods were used to achieve the objective. Historical and systemic methods were applied through analysis and synthesis, based on the review of bibliographic documents from academic and scientific databases.
From the empirical point of view, the scientific observation was carried out through a survey with nine dimensions that covered RSE and competitiveness indicators, measured through 45 items, in order to describe, verify and/or compare their behavior, association and possible adapted correlation, from the one applied by Marín and Rubio (2008).
Five-point Likert scales were used to measure the results. The survey was applied to the manager or administrator of each clinic; to validate the feasibility of the instrument, a pilot test was carried out on 10% of the sample through Alfa Cronbach, obtaining a value of 0.948, which corroborated the validity of the instrument.
For the calculation of the sample, the formula of the simple estimation method for random sampling was applied (Calero, 2003). The population of private health clinics in the Quito Metropolitan District was defined by their capacity for uninterrupted care and continuous care and hospitalization, with a total of 64 determined based on the Ministry of Public Health census. The remaining parameters defined were: significance level (á = 0.05); probability (p=0.5); error level (e=0.02). The calculated sample size was 58 private health clinics. The selection of the 58 clinics, which guaranteed randomness in the study, was made using a table of random numbers based on statistical studies and clinical trials, proposed by Lazcano et al. (2004).
The general index of RSE (IGRSE in Spanish) and competitiveness (IGC in Spanish) in the private clinics of the Quito Metropolitan District was measured through the dimensions and their items, respectively, proposed for RSE and competitiveness, obtaining the value of compliance for each clinic and, in general, for the sample determined through the mathematical formula for calculating the index (1), based on Oliveira, Hernández and do Rocío (2016).
![]() (1)
(1)
Where:
I = general compliance index
ΩD1 = weight of dimensions
VROD1 = value assigned by the respondent in the dimension
VMP = highest weighted value in the survey
The factorial analysis was applied in order to define the correlation between the dimensions of the variables, after calculating the correlation coefficient of Spearman's Rho between variables, calculation of the determinant, KMO and Bartlett's Sphericity Test. The factorial analysis allowed the generation of constructs of the most important relationships between RSE and competitiveness. For data processing, Microsoft Excel and IBM SPSS Statistics 22.
RESULTS AND DISCUSSION
RSE and competitiveness indices
Table 1 shows the statistical results of the general index of RSE compliance and competitiveness of the 58 private health clinics analyzed.
Table 1 - Statistical summary of general indexes of RSE compliance and competitiveness
|
RSE (IGRSE) |
COMPETITIVENESS (IGC) |
General index |
0,7893 |
0,6589 |
Standard deviation |
0,087 |
0,089 |
Xmin |
0,5747 |
0,4290 |
Xmax |
0,9787 |
0,8260 |
Source: Own elaboration from calculations made
As can be seen, the general RSE compliance index is 79%, with 98% being the highest and 58% the lowest. For its part, the competitiveness index was set at about 66%, with a minimum value of 43% and a maximum of 8.6%. The degree of dispersion or variability of the indices of the variables was measured, with RSE registering a standard deviation of 0.087 and competitiveness 0.089; in both cases, values close to zero denote low data dispersion.
Currently, RSE is implemented by companies to grow economically and position themselves socially in a context of competition where the impact on decision making and activities carried out by their employees on society and the environment must be recognized, always seeking ethical and transparent behavior (Molero García, 2017).
The RSE indices, as a strategic innovative indicator, mark the competitive capacity that the sector can have with respect to the environment and the means in which its resources are developed and the strategic relationship with other variables. Lau and Lukoki (2018), with regard to strategic relations in business management, indicate "...it constitutes the most general way of understanding the progress of business activity in an unpredictable and difficult environment, which requires concentration on those objectives that can be achieved and on the businesses, markets and areas to compete in, so that the capacity to respond effectively and efficiently to favourable opportunities and to threats or challenges is developed". The results obtained demonstrate medium-high levels of both RSE and competitiveness in Quito's private health clinics.
The general indexes of RSE compliance and competitiveness, identified zonally by the location of the clinics in the city of Quito, are shown in Table 2. The sectorization of the health system in Quito has been delimited by the Health Statistics Yearbook: Resources and Activities based on its geographic location, demographic profile, and participatory environment of health actors (INEC, 2014).
Table 2 - General indexes of RSE compliance and competitiveness, sectored in the Quito Metropolitan District
|
RSE INDEX (IGRSE) |
COMPETITIVENESS INDEX (IGC) |
North |
0,7860 |
0,6560 |
Center |
0,7929 |
0,6614 |
South |
0,8033 |
0,6692 |
Standard deviation |
0,0087 |
0,0066 |
Source: Own elaboration by analysis of results
In the north of the city, RSE index is 79%, in the center of the city 79% and in the south 80%. While in the case of competitiveness, in the north of the city, it has a competitiveness index of 66%, with similar data in the center and south. As can be seen, the values of RSE and competitiveness indices are similar in the three sectors of the city, with a standard deviation value in both cases close to zero.
Factorial analysis of RSE and competitiveness
The Spearman Rho coefficient was calculated for the 45 variables included in the survey, from which 13 of the variables with the least significance were extracted, determining the 32 variables with significant correlations that allowed the analysis to continue. The calculated determinant turned out to be a positive value other than zero, indicating that strong relationships exist between the variables.
The Kaiser-Meyer-Olkin coefficient (KMO) was also calculated, and a value of 0.70 was determined, which is favorable in terms of the feasibility of the components to be established with the corresponding constructs.
To determine and corroborate the application of the factorial analysis, the Bartlett Sphericity Test was also applied, with a value of 0.00, which allows the rejection of the null or initial hypothesis (H0), thus accepting the correlation between the variables studied.
Table 3 shows the variance calculated for the 32 variables or components.
Table 3 - Total variance explained by variables
Component |
Total |
% of variance |
% accumulated |
1 |
11,454 |
33,689 |
33,689 |
2 |
2,505 |
7,367 |
41,057 |
3 |
1,901 |
5,591 |
46,648 |
4 |
1,552 |
4,565 |
51,214 |
5 |
1,421 |
4,179 |
55,392 |
6 |
1,305 |
3,839 |
59,231 |
7 |
1,224 |
3,599 |
62,830 |
8 |
1,134 |
3,336 |
66,166 |
9 |
1,088 |
3,200 |
69,366 |
10 |
1,050 |
3,088 |
72,454 |
11 |
,891 |
2,622 |
75,076 |
12 |
,856 |
2,518 |
77,594 |
13 |
,841 |
2,475 |
80,069 |
14 |
,763 |
2,245 |
82,314 |
15 |
,669 |
1,968 |
84,282 |
16 |
,664 |
1,954 |
86,236 |
17 |
,590 |
1,736 |
87,972 |
18 |
,560 |
1,647 |
89,619 |
19 |
,453 |
1,333 |
90,952 |
20 |
,406 |
1,193 |
92,145 |
21 |
,377 |
1,110 |
93,255 |
22 |
,345 |
1,016 |
94,271 |
23 |
,315 |
,926 |
95,196 |
24 |
,287 |
,843 |
96,040 |
25 |
,257 |
,756 |
96,795 |
26 |
,234 |
,687 |
97,482 |
27 |
,210 |
,618 |
98,100 |
28 |
,160 |
,472 |
98,572 |
29 |
,140 |
,412 |
98,983 |
30 |
,105 |
,308 |
99,291 |
31 |
,095 |
,281 |
99,572 |
32 |
,069 |
,204 |
99,776 |
Source: Own elaboration from statistical analysis
As can be seen, in the first 10 components, approximately 70% of the accumulated variance is reached, which is ratified through the sedimentation graph, noting that it is the same 10 components that are located above the value of 1 (Fig. 1).
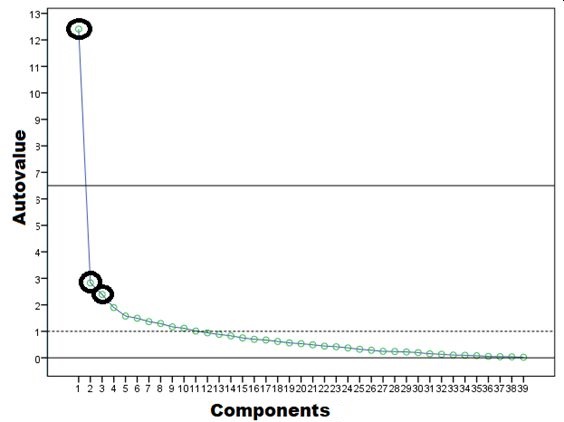
Fig. 1 - Sedimentation graph and suggested relation components
Source: Own preparation based on statistical analysis
The graph also allows us to determine that from component six onwards they maintain a constant with no major difference, therefore, the highest and most dispersed values are taken, which suggests that in three components there are the strongest correlations between RSE and competitiveness, this being the appropriate number of constructs to generate.
The above is ratified by the component analysis matrix shown below, where six constructs were studied, determining that it is in three of them where the variances are greater than 0.7 and relations are established between at least five variables.
Table 4 - Component analysis matrix
|
Component |
|||||
1 |
2 |
3 |
4 |
5 |
6 |
|
RSE1.20 |
0,8 |
0,1 |
0,2 |
0,2 |
0,0 |
-0,1 |
RSE1.16 |
0,7 |
0,2 |
0,2 |
0,2 |
0,0 |
0,0 |
RSE1.14 |
0,7 |
0,2 |
0,1 |
0,0 |
0,2 |
0,1 |
RSE1.19 |
0,7 |
0,3 |
0,0 |
0,0 |
0,1 |
-0,1 |
RSE1.3 |
0,7 |
0,2 |
0,0 |
0,2 |
-0,2 |
-0,1 |
RSE1.15 |
0,7 |
0,0 |
0,0 |
0,1 |
0,0 |
0,1 |
C1.2 |
0,7 |
0,1 |
0,2 |
0,3 |
0,0 |
0,2 |
C1.19 |
0,6 |
0,5 |
0,1 |
-0,1 |
0,1 |
0,1 |
RSE1.4 |
0,6 |
0,2 |
0,0 |
0,1 |
0,0 |
0,3 |
RSE1.24 |
0,6 |
0,3 |
0,3 |
0,0 |
0,1 |
0,1 |
RSE1.2 |
0,6 |
0,1 |
0,3 |
-0,1 |
-0,1 |
-0,2 |
RSE1.5 |
0,6 |
0,2 |
0,3 |
-0,1 |
0,0 |
0,2 |
RSE1.18 |
0,6 |
0,1 |
0,0 |
0,4 |
0,2 |
-0,3 |
RSE1.17 |
0,6 |
0,2 |
0,1 |
0,4 |
0,2 |
0,1 |
RSE1.8 |
0,4 |
0,2 |
0,2 |
0,3 |
0,1 |
0,3 |
C1.17 |
0,1 |
0,7 |
0,0 |
0,1 |
0,1 |
0,0 |
C1.9 |
0,2 |
0,6 |
0,1 |
0,1 |
0,1 |
0,0 |
C1.7 |
0,1 |
0,6 |
0,1 |
0,3 |
-0,2 |
0,1 |
C1.8 |
0,1 |
0,6 |
0,2 |
0,4 |
-0,2 |
0,1 |
C1.15 |
0,4 |
0,6 |
0,2 |
0,1 |
0,1 |
0,0 |
C1.18 |
0,5 |
0,6 |
0,0 |
-0,1 |
0,0 |
0,1 |
C1.14 |
0,2 |
0,5 |
0,1 |
0,0 |
0,4 |
-0,2 |
C1.16 |
0,5 |
0,5 |
-0,1 |
0,3 |
0,0 |
0,1 |
C1.13 |
0,4 |
0,5 |
0,3 |
-0,1 |
-0,3 |
0,1 |
C1.1 |
0,4 |
0,5 |
0,3 |
0,5 |
0,1 |
-0,1 |
RSE1.21 |
0,3 |
0,5 |
0,3 |
-0,1 |
0,0 |
0,1 |
C1.10 |
0,2 |
0,4 |
0,1 |
0,3 |
-0,2 |
0,3 |
C1.4 |
0,3 |
0,1 |
0,7 |
-0,1 |
0,0 |
0,2 |
RSE1.7 |
0,0 |
0,0 |
0,6 |
0,3 |
0,1 |
0,0 |
C1.6 |
0,1 |
0,1 |
0,6 |
0,4 |
0,0 |
-0,1 |
C1.11 |
0,1 |
0,6 |
0,6 |
0,0 |
0,0 |
0,0 |
C1.3 |
0,2 |
0,1 |
0,6 |
0,2 |
-0,1 |
0,1 |
C1.5 |
0,4 |
0,2 |
0,5 |
0,1 |
-0,1 |
0,1 |
RSE1.1 |
0,1 |
0,2 |
0,5 |
-0,1 |
0,3 |
-0,3 |
RSE1.6 |
0,1 |
0,2 |
0,3 |
-0,2 |
0,0 |
0,2 |
Source: Own preparation based on statistical analysis
Based on the above analysis, the following table of components or constructs is generated:
Table 5 - Elaboration of the constructs from the analysis of the main components
Component |
Constructs |
Items |
Total |
RC 1 |
Levels of RSE, active participation in the community |
RSE1.20, RSE1.16, RSE1.14, RSE1.19, RSE1.3, RSE1.15, C1.2, C1.19, RSE1.4, RSE1.24, RSE1.2, RSE1.5, RSE1.18, RSE1.17, RSE1.8 |
15 |
RC 2 |
Internal and external results and organizational structure |
C1.17, C1.9, C1.7, C1.8, C1.15, C1.18, C1.14, C1.16, C1.13, C1.1, RSE1.21, C1.10 |
12 |
RC 3 |
Labor practices and innovation |
C1.4, RSE1.7, C1.6, C1.11, C1.3, C1.5, RSE1.1, RSE1.6 |
8 |
Source: Own preparation based on statistical analysis
Each construct has been established with the questions or items with positive correlation values ranging from 0.31 to 0.79, as shown in the component matrix (Table 4). The following constructs have been established based on nine dimensions that evaluate RSE and competitiveness in Quito's private clinics:
The RC1 construct corresponds to the items referring to the levels of RSE and the active participation of the clinics in the community, which makes it clear that the consideration, implementation and practice of RSE principles are fundamental to the good performance of private health clinics, but, above all, that it makes them more competitive, with a more responsible image and commitment to the actors linked to the institution. This proposal for the fulfillment of RSE starts from the philosophy, mission and vision that the clinic proposes with its collaborators. RSE, due to its diverse interpretations, conditions its perspective or action; the actions taken in social development and well-being of the communities structure new criteria of participation and responsible practices, seeking the joint development of the people (Mori Sánchez, 2009).
The RC2 construct corresponds to the organizational structure and its internal and external results. Today, organizations are immersed in a dizzying environment, for which it is necessary to incorporate a solid organizational structure with differentiating proposals and procedures in the face of changes in organizational work, seeking to translate these changes into economic growth (Ferrer, 2016). This is a consistent relationship, but one of great importance in the performance of private institutions in the health sector. A private clinic, with a solid organizational structure, with well-defined functions and processes, will delineate the results obtained; if the clinic proposes and manages a solid structure, its internal and external results will be reflected in an orchestrated and controlled development, giving greater possibility to be a reference in the sector.
The RC3 construct corresponds to RSE in labor practices and innovation. Research has shown that the correct implementation, control and management of working practices makes clinics more competitive, since, together with innovation, they generate a different value in the development of activities, seeking to make innovation an elemental tool of differentiation in the market. Access to new technologies, simplified and effective activities, have outlined the competitiveness of the clinics among themselves, making us assume that the customer segment that each of these institutions has in its portfolio also depends on this construct.
In conclusion, it is recognized that the private health clinics in the Quito Metropolitan District show a favorable index of RSE compliance, while the competitiveness index is lower than that of RSE. Furthermore, similar behavior was shown in the three sectors of the city (north, center and south) with regard to RSE and competitiveness indices.
The application of the factor analysis made it possible to determine three fundamental components in the relationship between RSE and competitiveness in Quito's private clinics: levels of RSE, with active participation in the community; internal and external results of organizational structure and labor practices and innovation.
With regard to the levels of RSE and active participation in the community, it was concluded that there is a high level of RSE in all the indicators linked to internal organization and participation with the community. With respect to the internal and external results of organizational structure, it is concluded that a solid organizational structure can consolidate a strong and flexible organization to the demands, obtaining results for its internal and external actors. Labor practices and innovation are determining factors in achieving high levels of competitiveness.
REFERENCES
Calero, A. (2003). Estadística III. Félix Varela.
Coba Molina, E., Díaz Córdova, J., Zurita Meza, E., & Proaño López, P. (2017). La responsabilidad social empresarial en las empresas del Ecuador. Un test de relación con la imagen corporativa y desempeño financiero. Ingeniería Industrial. Actualidad y Nuevas Tendencias, 5(18), 23-44. http://servicio.bc.uc.edu.ve/ingenieria/revista/Inge-Industrial/volv-n18/art02.pdf
Duarte, F. (2015). Responsabilidad social empresarial. Revista Lidera, (10), 41-45. http://revistas.pucp.edu.pe/index.php/revistalidera/article/view/18221
Duque Orozco, Y. V., Cardona Acevedo, M. de la M., & Rendón Acevedo, J. A. (2013). Responsabilidad Social Empresarial: Teorías, índices, estándares y certificaciones. Cuadernos de Administración, 29(50), 196-206. https://doi.org/10.25100/cdea.v29i50.55
Fernández, A., Calero, S., Parra, H., & Fernández, R. (2017). Corporate social responsibility and the transformation of the productive matrix for Ecuador sustainability. Journal of Security and Sustainability Issues, 6(4), 575-584. https://doi.org/10.9770/jssi.2017.6.4(4)
Ferrer, M. A. (2016). Innovación y diseño organizacional. Revista Venezolana de Gerencia, 21(74), 190-192. https://doi.org/10.37960/revista.v21i74.21254
Gómez Perdomo, D. A. (2018). Modelo teórico de indicadores de responsabilidad social en salud. Pensamiento y Acción Interdisciplinaria, 4(1), 8-24. https://doi.org/10.29035/pai.4.1.8
INEC. (2014). Anuario de Estadística de Salud: Recursos y actividades. Instituto Nacional de Estadísticas y Censos.
Lau Rodríguez, C. B., & Lukoki, E. (2018). El perfeccionamiento estratégico y la estrategia de disminución del costo de inversión petrolera en la empresa Sonangol Cuba. Cofín Habana, 12(2), 381-394. http://www.cofinhab.uh.cu/index.php/RCCF/article/view/321
Lazcano Ponce, E., Salazar Martínez, E., Gutiérrez Castrellón, P., Ángeles Llerenas, A., Hernández Garduño, A., & Viramontes, J. L. (2004). Ensayos clínicos aleatorizados: Variantes, métodos de aleatorización, análisis, consideraciones éticas y regulación. Salud Pública de México, 46(6), 559-584. http://saludpublica.mx/index.php/spm/article/view/6579
Luciani Toro, L. R., & Navarro Silva, O. (2018). Los Sistemas de Información en la competitividad de las pequeñas y medianas empresas. Universidad y Sociedad, 10(2), 139-144. https://rus.ucf.edu.cu/index.php/rus/article/view/837
Marín Rives, L., & Rubio Bañón, A. (2008). La responsabilidad social corporativa como determinante del éxito competitivo: Un análisis empírico. Revista Europea de Dirección y Economía de la Empresa, 17(3), 27-42. https://dialnet.unirioja.es/servlet/articulo?codigo=2725440
Molero García, G. J. (2017). La responsabilidad social empresarial en el contexto del capital social. Omnia, 22(3), 46-59. https://produccioncientificaluz.org/index.php/omnia/article/view/22581
Morales-Guzmán-Barró, R. (2014). Iniciativas de responsabilidad social por empresas y universidades en áreas de salud pública. Revista de la Sociedad Peruana de Medicina Interna, 27(2), 95-98.
Mori Sánchez, M. del P. (2009). Responsabilidad social: Una mirada desde la psicología comunitaria. Liberabit, 15(2), 163-170. http://pepsic.bvsalud.org/scielo.php?script=sci_abstract&pid=S1729-48272009000200010&lng=pt&nrm=iso&tlng=es
Naranjo Arango, R., Mercado Caruso, N., Naranjo Del Giudice, O., & Giraldo Oliveros, M. E. (2018). Responsabilidad Social Empresarial (RSE) en medianas empresas del departamento del Atlántico, Colombia. Revista Venezolana de Gerencia, 23(84), 913-927. https://www.produccioncientificaluz.org/index.php/rvg/article/view/24252
Oliveira Sencioles, S. V., Hernández Santoyo, A., & do Rocio Strauhs, F. (2016). Use of Wikis in Organizational Knowledge Management. Social Networking, 5(1), 39-56. https://doi.org/10.4236/sn.2016.51005
Reficco, E., & Marquina Feldman, P. (2015). Impacto de la responsabilidad social empresarial en el comportamiento de compra y disposición a pagar de consumidores bogotanos. Estudios Gerenciales, 31(137), 373-382. https://doi.org/10.1016/j.estger.2015.10.001
Ruiz de Chávez, M. H. (2016). Temas selectos de CONBIOÉTICA. Comisión Nacional de Bioética. http://www.conbioeticamexico.salud.gob.mx/descargas/pdf/registrocomites/Temas_Selectos_de_CONBIOETICA.pdf
Terán Rosero, G. J., Montenegro Obando, B. L., Bastidas Guerrón, J. L., Realpe Cabrera, I. A., Villarreal Salazar, F. J., & Fernández Lorenzo, A. (2017). Análisis crítico de la responsabilidad social en entidades de salud. Revista Cubana de Investigaciones Biomédicas, 36(1), 1-10. http://scielo.sld.cu/scielo.php?script=sci_abstract&pid=S0864-03002017000100020&lng=es&nrm=iso&tlng=es
Vásquez Fajardo, C. E., Pérez Salazar, J. A., Fajardo Vaca, L. M., Scrich Vázquez, A. J., & Cruz Fonseca, L. de los Á. (2018). El tratamiento de la salud pública y ambiental desde la responsabilidad social empresarial en Ecuador. Archivo Médico Camagüey, 22(3), 366-380. http://www.revistaamc.sld.cu/index.php/amc/article/view/5633
Conflict of interest:
Authors declare not to have any conflict of interest.
Authors' contribution:
The authors have participated in the writing of the paper and the analysis of the documents.
